Article Text

Abstract
Aims To compare the refractive and visual outcomes of femtosecond laser-assisted astigmatic keratotomy (FSAK) and toric intraocular lens (IOL) implantation for correcting astigmatism in cataract patients.
Methods Studies were retrieved from the Ovid-Medline, EMBASE, Cochrane Central Register of Controlled Trials and Scopus which compared FSAK and toric IOL for astigmatism correction in cataract patients. Outcome measures included postoperative refractive cylinder, correction index, uncorrected distance visual acuity (UDVA), the proportion of patients achieving a residual refractive cylinder of 1.00 dioptre or less, target-induced astigmatism (TIA) and surgically induced astigmatism (SIA). The trial sequential analysis (TSA) was used to collect firm evidence supporting our conclusion.
Results 9 studies encompassing 590 participants were analysed. The meta-analysis revealed that toric IOLs could result in less postoperative refractive cylinder and provide better UDVA compared with FSAK. The TSA disclosed strong evidence of lower postoperative refractive cylinder in the toric IOL group compared with that of the FSAK group. FSAK showed a smaller correction index and lower mean TIA and SIA compared with toric IOLs.
Conclusions For cataract patients, both FSAK and toric IOLs are effective methods for correcting astigmatism. However, toric IOLs offer less postoperative astigmatism and result in better postoperative UDVA compared with FSAK. In vector analysis of astigmatism, toric IOLs can also produce higher TIA and SIA. Additionally, neither method is associated with severe untreatable complications. Therefore, the conclusion is that toric IOLs are the preferred choice for astigmatism correction in cataract patients and FSAK serves as a viable alternative when toric IOLs are contraindicated.
- Ophthalmologic Surgical Procedures
- Cornea
- Optics and Refraction
- Treatment Lasers
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Both femtosecond laser-assisted astigmatic keratotomy (FSAK) and toric intraocular lens (IOL) implantation have recently become popular to correct astigmatism in cataract patients, but no consensus on which technique is better has been reached.
WHAT THIS STUDY ADDS
The study revealed that toric IOLs could result in less postoperative refractive cylinder and provide better uncorrected distance visual acuity (UDVA) compared with FSAK, and these results were statistically significant. Furthermore, the trial sequential analysis (TSA) disclosed strong evidence of lower postoperative refractive cylinder in the toric IOL group compared with that of the FSAK group.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
This study found that toric IOLs, compared with FSAK, result in significantly less postoperative refractive cylinder and provide better UDVA. The TSA results provide robust evidence confirming that toric IOLs indeed generate less postoperative refractive cylinder. Subsequent research may no longer need to focus on comparing toric IOL and FSAK for postoperative refractive cylinder. On the other hand, the study provided the results of vector analysis of astigmatism between FSAK and toric IOLs.
Introduction
Cataract surgery is one of the common procedures in the field of ophthalmology, with the aim of removing cataracts in the eye to restore vision and improve visual quality. Furthermore, the improvement of vision after cataract surgery relies on the achievement of emmetropia.1 2 Factors influencing postcataract surgery emmetropia could include residual astigmatism or errors in the calculation of intraocular lens (IOL) power.3 Nearly 70% of cataract patients have corneal astigmatism ranging from 0.5 dioptres (D) to 1.25 D preoperatively, while around 20% of patients have corneal astigmatism exceeding 1.25 D.4 5 A review has indicated that 15%–56% of postcataract surgery patients experience astigmatism of 1 D or more.6 Moreover, the presence of postoperative astigmatism still remains one of the factors contributing to poor vision after cataract surgery.1 As a result, numerous methods have been employed to decrease preoperative corneal astigmatism in cataract patients, such as limbal relaxing incisions,7 8 arcuate keratotomy (AK)9 and the more recently popular toric intraocular lens.10
Toric IOLs are specialised implants used in cataract surgery to correct astigmatism. Certainly, toric IOLs have gained importance as a significant approach for correcting pre-existing astigmatism in cataract patients due to their higher predictability, improved contrast sensitivity, greater spectacle independence and suitability for higher levels of astigmatism.10 11 However, there are certain specific contraindications and considerations related to toric IOLs. Toric IOLs are designed to correct astigmatism by aligning specific meridians of the lens with the axis of astigmatism in the patient’s eye. If a toric IOL rotates after surgery, it can affect the accuracy of astigmatism correction and lead to suboptimal visual outcomes.11
Therefore, while toric IOLs offer numerous benefits for astigmatism correction, there are cases where the risk of IOL rotation could make other options more suitable. In situations where a patient is at a higher risk of IOL rotation, such as in cases with post-traumatic eyes or eyes with long axial lengths, addressing astigmatism on the corneal surface through other methods can be an alternative choice.11
AK is a surgical procedure used to correct astigmatism by making precise incisions in the cornea, which is often performed by a specialised instrument or a laser.12 13 Because the femtosecond laser technology can accurately create corneal incisions, it is also used in conjunction with AK to enhance the precision and predictability of the procedure.12 The increasing popularity of femtosecond laser-assisted astigmatic keratotomy (FSAK) is indeed influenced by the growing prevalence of femtosecond laser-assisted cataract surgery.12
Similar meta-analyses in the past have found that toric IOLs provide better visual acuity and less residual astigmatism compared with corneal relaxing incisions.14 15 Recently published meta-analysis by Zheng et al also found that toric IOLs have less residual postoperative astigmatism, but there is no significant difference in uncorrected distance visual acuity (UDVA).16 Recently, numerous studies have provided updated information on postoperative residual astigmatism and visual outcomes between toric IOLs and FSAK after cataract surgery.13 17–25 Therefore, this study primarily focuses on data up until December 2023, comparing the various refractive and visual outcomes of FSAK and toric IOLs for correcting astigmatism in cataract patients.
Methods
Literature search
The current study followed the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-analyses.26 EMBASE, Ovid-Medline, Cochrane Central Register of Controlled Trials and Scopus databases were searched systematically to identify relevant studies. The last literature search was performed on 10 December 2023 by W-TY. This present search primarily used key terms such as ‘femtosecond laser’, ‘toric IOL‘ and ‘astigmatic keratotomy’. For a comprehensive view of the search syntax, refer to online supplemental eTable 1.
Supplemental material
Inclusion/exclusion criteria
The inclusion of studies was based on the following criteria: (1) randomised controlled trial (RCT) and observational studies, (2) adult patients with cataract and astigmatism, (3) comparison of FSAK and toric IOL for correcting astigmatism and (4) reported at least one clinical outcome, such as postoperative refractive cylinder, correction index, UDVA, target-induced astigmatism (TIA) and surgically induced astigmatism (SIA). The exclusion criteria were as follows: (1) phase I and II clinical trials and (2) studies where AK was not performed using a femtosecond laser. The selection of articles for inclusion was independently conducted by W-TY and Y-MC, employing EndNote V.X9 for the screening process.
Data extraction and quality assessment
Data from the included studies were extracted by two authors, W-TY and Y-MC, using Microsoft Excel for organised data management. The extraction process involved tabulating various parameters in an Excel spreadsheet, including author, publication year, study method, country, FSAK process, femtosecond laser system, types of IOL, sample size and follow-up duration. The risk of bias in the eligible RCTs was independently assessed using the Cochrane Risk-of-Bias Tool for Randomized Trials (RoB 2),27 while the risk of bias in observational studies was evaluated using the Risk Of Bias In Non-randomized Studies of Interventions (ROBINS-I) tool,28 with assessments conducted by both W-TY and Y-MC. In cases of disagreement concerning bias risk, the conclusive decision was made by T-HW, guided by the protocols outlined in the Cochrane Reviewer’s Handbook.29
Data synthesis and analysis
The meta-analysis was conducted using Review Manager 5.4 software. The postoperative refractive cylinder, correction index, UDVA, TIA and SIA were analysed as continuous variables, and the outcome measurements were reported as the mean difference (MD) with a 95% CI. The proportion of patients achieving a residual refractive cylinder of 1.00 D or less was analysed as a dichotomous variable, with outcome measurements expressed as ORs and a 95% CI. P<0.05 was regarded as statistically significant. The study’s heterogeneity was evaluated using the I square (I2) and Q test analyses. Significant heterogeneity was identified when p<0.10 and I2>50%. The presence of publication bias was investigated through funnel plots. For the synthesis of continuous and dichotomous variables, the study employed the inverse variance method and the Mantel-Haenszel method, respectively. Finally, the present meta-analysis integrated current available studies and performed trial sequential analysis (TSA) using TSA software V.0.9.5.10 beta for the calculation.30
Results
Literature search
Figure 1 provides a summary of the literature search process. After reviewing 678 articles from electronic databases, subsequently, 12 full-text articles were scrutinised for their suitability. Ultimately, nine studies, which comprised two RCTs and seven observational studies, were selected for the quantitative meta-analysis. Online supplemental eTable 1 outlines the comprehensive search strategies, procedures and findings.

Flowchart of study selection process.
Characteristics of the eligible studies
The characteristics of the nine included studies are summarised in table 1. The cumulative sample size of included studies was 590 participants, with the combined experimental and control group sizes in individual studies ranging from 44 to 94 subjects. Follow-up durations varied from 3 months to 12 months, which allowed for the evaluation of postoperative visual acuities and refractive outcomes.
Characteristics of included clinical studies regarding the comparison of femtosecond laser-assisted astigmatism and toric IOLs for correcting astigmatism in cataract
Interventional strategies employed across the studies were heterogeneous, utilising a spectrum of femtosecond laser platforms such as the Catalys (Abbott), IntraLase (Abbott), Victus (Bausch + Lomb), LenSx (Alcon) and Lensar (Ally) system. The control arms in these studies were characterised by the implantation of toric IOLs, with a selection of lenses from noted manufacturers such as Abbott Medical Optics, Rayner, Bausch + Lomb and Alcon, predicated on meticulous preoperative planning and intraoperative calibrations.
Quality of the included studied
For the two RCTs, the Cochrane Risk of Bias 2.0 tool was employed,27 whereas the seven non-RCTs were evaluated using the Cochrane ROBINS-I tool.28 The results of the quality assessment are organised in online supplemental eFigures 1 and 2.
The RCTs conducted by Shaarawy18 and Hernandez19 displayed some concerns in the randomisation process and the selection of the reported results. However, both studies were deemed to have a low risk of bias in deviations from intended interventions, missing outcome data and measurement of the outcomes, suggesting that the conducted interventions and the reporting of outcomes were generally consistent and reliable.
In contrast, the retrospective and prospective cohort studies, which included research by Yoo et al, Kwon et al, Noh et al, Lin et al, Wang nd Chen, Shen et al and Yuan et al,17 20–25 exhibited a moderate risk of bias due to confounding. Despite this, the selection of participants in the study, the classification of interventions and deviations from intended interventions were generally associated with a low risk of bias. However, except for Yoo et al and Lin et al,17 22 the remaining studies exhibited moderate risks concerning the selection of the reported results.
The overall risk of bias was categorised as moderate for the majority of non-RCTs, except for Shen et al,24 which was assessed to have a low risk of bias.
Primary outcomes
Postoperative refractive cylinder
A total of 533 patients from 1 RCT and 7 observational studies were included to estimate the weighted MD (WMD) of postoperative refractive cylinder (figure 2A). In the subgroup analysis of the simultaneous group, toric IOLs exhibited a lower postoperative refractive cylinder compared with FSAK (WMD=0.20; 95% CI (0.14 to 0.25)). However, in the delayed group, FSAK showed a lower postoperative refractive cylinder (WMD=−0.05; 95% CI (−0.11 to 0.00)). Overall, the meta-analysis revealed that patients receiving toric IOLs had a slightly lower postoperative refractive cylinder compared with those who received FSAK (WMD=0.17; 95% CI (0.05, 0.29)). The funnel plot for the outcome of postoperative refractive cylinder is shown in online supplemental eFigure 3.

(A) Forest plot of postoperative refractive cylinder comparing FSAK and toric IOL groups. The forest plot revealed that patients receiving toric IOLs had a slightly lower postoperative refractive cylinder compared with those who received FSAK (WMD=0.17; 95% CI (0.05 to 0.29)). IOL, intraocular lens; FSAK, femtosecond laser-assisted astigmatic keratotomy; WMD, weighted mean difference (B) Trial sequential analysis (TSA) of nine trials comparing postoperative refractive cylinders between the FSAK and toric IOL groups. The cumulative z curve crossed the trial sequential monitoring boundary and disclosed strong evidence of lower postoperative refractive cylinder in the toric IOL group compared with that of the FSAK group. IOL, intraocular lens; FSAK, femtosecond laser-assisted astigmatic keratotomy.
Trial sequential analysis
The TSA (figure 2B) for postoperative refractive cylinder was conducted with a required information size (RIS) of 467 eyes to achieve a power of 80% and maintain a type I error rate of 5%. The present meta-analysis, encompassing a total of 533 eyes, met the estimated RIS, providing a robust sample size for the TSA. The cumulative Z curve crossed the trial sequential monitoring boundary, indicating a significant reduction in postoperative refractive cylinder favouring the toric IOL group over the FSAK group. This crossing of the boundary suggests conclusive evidence that toric IOLs are superior to FSAK for reducing postoperative refractive cylinder, supporting the sufficiency of the data collected and potentially obviating the need for further trials on this outcome. TSA, excluding the study by Yoo et al,17 showed similar results, as depicted in online supplemental eFigure 4.
Secondary outcomes
Correction index
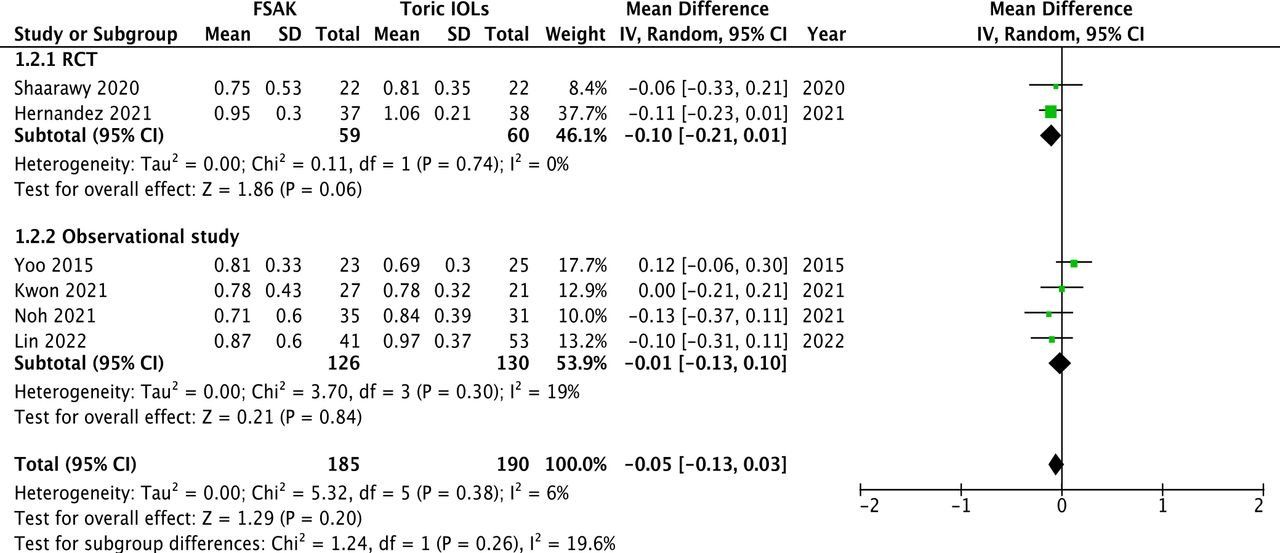
Pooled data from 375 eyes across 6 studies were obtained to evaluate the WMD of the correction index following FSAK and toric IOLs. The analysis was stratified into two subgroups: RCTs and observational studies (figure 3).

Forest plot of the correction index comparing FSAK and toric IOL groups. Subgroup analysis of different study designs in correction index. From the RCT subgroup, the FSAK group showed a smaller correction index compared with the toric IOL group (WMD=−0.10; 95% CI (−0.21 to 0.01)). Similarly, the observational study subgroup demonstrated a lower correction index in FSAK group compared with toric IOL group (WMD=−0.01; 95% CI (−0.13 to 0.10)). IOL, intraocular lens; FSAK, femtosecond laser-assisted astigmatic keratotomy; RCT, randomised controlled trial; WMD, weighted mean difference.
From the RCT subgroup, which included 59 eyes from 2 studies, the FSAK group showed a smaller correction index compared with the toric IOL group (WMD=−0.10; 95% CI (−0.21 to 0.01)). Similarly, the observational study subgroup, comprising 316 eyes from 4 studies, demonstrated a lower correction index in FSAK group compared with toric IOL group (WMD=−0.01; 95% CI (−0.13 to 0.10)). When considering the total pooled data from both subgroups, the overall WMD was −0.05 (95% CI −0.13 to 0.03).
Postoperative UDVA
A total of 419 eyes from six studies were analysed to compare the WMD in postoperative UDVA between FSAK and toric IOLs. The combined results showed a slight advantage for toric IOLs over FSAK, with a WMD of 0.07 (95% CI 0.00 to 0.13) (figure 4A).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plots of the visual and refractive outcomes comparing FSAK and toric IOL groups. (A) Postoperative UDVA. (B) Residual refractive cylinder of 1.0 D or less. (C) TIA. (D) SIA. (A) Postoperative UDVA. The forest plot showed a slight advantage for toric IOLs over FSAK, with a WMD of 0.07 (95% CI 0.00 to 0.13). (B) Residual refractive cylinder of 1.0 D or less. The forest plot demonstrated that FSAK had a lower chance of achieving a residual refractive cylinder of 1.00 D or less compared with those receiving toric IOLs (OR=0.23; 95% CI (0.09 to 0.63)). (C) TIA. The forest plot showed that FSAK was associated with a statistically significant lower mean TIA compared with toric IOLs (WMD=−0.48 D; 95% CI (−0.82 to –0.14)). (D) SIA. The pooled data indicated that FSAK was associated with a statistically significant lower SIA compared with toric IOLs (WMD=−0.46; 95% CI (−0.85 to –0.07)). IOL, intraocular lens; FSAK, femtosecond laser-assisted astigmatic keratotomy; WMD, weighted mean difference; UDVA, uncorrected distance visual acuity; TIA, target-induced astigmatism; SIA, surgically induced astigmatism
Residual refractive cylinder of 1.0 D or less
The pooled results of 3 included studies indicate that patients undergoing FSAK had a lower chance of achieving a residual refractive cylinder of 1.00 D or less compared with those receiving toric IOLs (OR=0.23; 95% CI (0.09 to 0.63)). This suggests that toric IOLs are more likely to result in a residual refractive cylinder of 1.00 D or less when compared with FSAK (figure 4B).
Target-induced astigmatism
The present meta-analysis examined the differences in TIA outcomes between FSAK and toric IOLs from a pool of 279 eyes across 4 studies. The aggregated data showed that FSAK was associated with a statistically significant lower mean TIA compared with toric IOLs (WMD=−0.48 D; 95% CI (−0.82 to –0.14)) (figure 4C).
Surgically induced astigmatism
The present meta-analysis evaluated the SIA across 375 eyes from 6 studies to compare the outcomes between FSAK and toric IOLs. The pooled data indicated that FSAK was associated with a statistically significant lower SIA compared with toric IOLs (WMD=−0.46; 95% CI (−0.85 to –0.07)) (figure 4D).
Discussion
There is a growing body of literature comparing the effectiveness of toric IOLs and FSAK in correcting astigmatism in cataract surgery patients. Therefore, the meta-analysis was conducted to compare the refractive and visual outcomes of FSAK and toric IOLs for astigmatism correction in cataract patients.
Postoperative astigmatism has consistently been a key factor affecting visual outcomes after cataract surgery.1 In the present meta-analysis, toric IOLs outperformed FSAK by significantly increasing the proportion of patients with <1.0 D of residual astigmatism and also showing lower average residual cylinder values. Furthermore, the present meta-analysis provides more statistically reliable results via TSA. Among the articles analysed, only one did not involve simultaneous cataract and FSAK surgery. Instead, this study first performed cataract surgery and then, 1 month postoperatively, performed FSAK to correct the patient’s postoperative astigmatism.17 Therefore, the study concluded that there was no difference in postoperative residual astigmatism between FSAK and toric IOLs.
Postoperative UDVA is another concerning issue following cataract surgery. The present analysis found that the toric IOL implantation provides better postoperative UDVA in comparison with FSAK and the result is significant. This meta-analysis includes six studies, with two studies showing no significant difference in postoperative UDVA between the two methods,22 25 while the other four studies suggest that toric IOL may offer better postop UDVA.17 19 23 24 The result is consistent with previous similar meta-analyses.14 15 It seems that toric IOL implantation may offer better postoperative UDVA compared with both manual and femtosecond laser-assisted corneal relaxing incisions. Such results are expected because reducing postoperative astigmatism can indeed lead to better postoperative UDVA.31
However, in contrast to the findings of a recently published meta-analysis by Zheng et al, which indicated no significant difference in UDVA between the toric IOL and FSAK groups,16 our meta-analysis suggests otherwise. This discrepancy may stem from our inclusion of more recent studies, resulting in a larger sample size that enhances the precision of our results.
Vector analysis of astigmatism was used to better understand the orientation and magnitude of astigmatism.32 In the current meta-analysis, a significant difference in TIA was observed between the toric IOLs and FSAK groups. The TIA in the toric IOL group was notably higher than that in the FSAK group. Furthermore, in terms of SIA, the toric IOL group exhibited a significant increase compared with the FSAK group. Hernandez et al believed that patients undergoing FSAK with greater preoperative astigmatism may require longer and deeper arcuate incisions. This could potentially impact the healing process of the corneal incision and consequently affect the effectiveness of astigmatism correction.19 Noh et al also found if a patient’s preoperative astigmatism is >1.5 D, in the FSAK group, the SIA may be significantly less than the TIA.21 Additionally, in the study by Hernandez et al, they observed that in the FSAK group, SIA and TIA were quite similar.19 One possible reason for this discrepancy could be attributed to differences in the handling of astigmatic keratotomy incisions. In the study by Noh et al, astigmatic keratotomy incisions were not opened, whereas in the study by Hernandez et al, they were opened.19 21 The variation in how the incisions were managed may contribute to the observed differences in SIA and TIA across different studies. Regarding the correction index, most articles, whether in toric IOLs or FSAK, demonstrated undercorrection in astigmatism correction, and the results were not statistically significant.17 18 20–22 However, Hernandez et al found overcorrection of refractive astigmatism in the toric IOL group and undercorrection in the FSAK group,19 but the result was not significant.
Regarding surgical complications, except for three articles that did not mention it,18 22 23 the other six articles17 19–21 24 25 reported no incidents of corneal ectasia, hyperopic shift or infectious keratitis in the FSAK group. In the toric IOL group, no IOL was misaligned more than 10°. The results aligned with previous meta-analyses14 15; neither toric IOLs nor limbal relaxing incisions resulted in permanent complications.
For FSAK, while immediate postoperative complications such as corneal ectasia and hyperopic shift were not reported in the reviewed literature, the possibility of late-onset complications such as infectious keratitis, especially in patients who underwent previous penetrating keratoplasty, and the overcorrection and regression of astigmatic correction warrant long-term surveillance.33 34 In the case of toric IOLs, the primary concern in the late postoperative period revolves around the potential for IOL rotation or displacement.15
Although subjected to a detailed review, this meta-analysis still had some limitations. First, this present study only included nine studies (two RCTs and seven cohort studies), which could have influenced the reliability and validity of the study. Second, the varying follow-up times in each article may introduce a limitation to this meta-analysis. The analysis relied on the final follow-up time of each article, and this variability in follow-up times could potentially impact the statistical outcomes. Third, the differences in laser surgical machines, variations in the surgical techniques and the distinct surgical nomograms referenced for AK within the FSAK group could affect the assessment of the results. Fourth, the analysis in the articles considered has shown that astigmatism does not exceed 4.5 D. It is hoped that in the future, studies involving higher levels of astigmatism can be included to conduct subgroup analyses. This would help understand whether different degrees of astigmatism also impact the astigmatism correction outcomes of these two surgical methods. In conclusion, in both vector analysis and arithmetic analysis, toric IOL correction tends to address more astigmatism and results in less residual astigmatism compared with FSAK. Furthermore, toric IOLs can provide better UDVA in comparison with FSAK. However, there is no significant difference in postoperative complications between the two methods. Therefore, toric IOLs are the preferred choice for astigmatism correction in cataract patients, and FSAK serves as a viable alternative when toric IOLs are contraindicated.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors Y-MC was the guarantor of the study. W-TY and Y-MC conceived and designed the study. W-TY, T-HW and Y-MC contributed to database search, data extraction and quality assessment. W-TY and Y-MC performed the meta-analysis and wrote the first draft of the study. W-TY, T-YL, M-CT, Y-HC and Y-MC contributed to the interpretation of data analysis and critical revision of the manuscript. Y-MC supervised the whole study process. All authors contributed to and approved the final manuscript. All authors met the ICMJE criteria for authorship.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.