Article Text

Abstract
Background/aims To identify the risk factors for neuropathic corneal pain (NCP) following corneal refractive surgery and to report its clinical manifestations, imaging and proteomic characteristics.
Methods This 1 year prospective cohort study included 100 eyes that underwent small incision lenticule extraction (SMILE) or laser-assisted in situ keratomileusis (LASIK). Ocular surface assessments, in-vivo confocal microscopy scans, tear neuromediators and proteomics analyses were performed. NCP was assessed using the ocular pain assessment survey. Univariate and multivariate analyses were conducted to identify the risk factors associated with postoperative NCP.
Results The incidence of NCP was 13.3% and 10.5% after SMILE and LASIK, respectively (p=0.70). In SMILE, preoperative manifest refractive spherical equivalent (MRSE) and spherical power (both p=0.02) were significantly higher in the NCP compared with the non-NCP group. In LASIK, NCP eyes had a significantly lower corneal nerve fibre length (CNFL) (p=0.02), lower nerve fractal dimension (p=0.003), higher nerve fibre width (p=0.04) and larger neuroma area (p=0.04) than non-NCP eyes. In SMILE, higher preoperative MRSE was a significant risk factor for postoperative NCP (95% CI: 0.48—1.96, p=0.04). An MRSE greater than −8.0 diopter was 9.57 times more likely to develop postoperative NCP (OR=9.57, p=0.002). In LASIK, lower preoperative corneal nerve fibre density (95% CI:0.13—1.11, p=0.05) and CNFL (95% CI:0.09—1.25, p=0.05) were significant risk factors for postoperative NCP. Significant increases in tear nerve growth factor, calcitonin gene-related peptide, Frizzled class receptor 7 and nucleoside-diphosphate kinase three were observed in postoperative NCP.
Conclusions The reported characteristics and risk factors would identify patients susceptible to NCP after corneal refractive surgery.
- Risk Factors
- Cornea
- Ocular surface
- Ophthalmologic Surgical Procedures
Data availability statement
Data are available upon reasonable request. Data will be made available upon request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Neuropathic corneal pain (NCP) following refractive surgery is debilitating. However, the incidence of NCP after small incision lenticule extraction (SMILE), as well as the risk factors and molecular data on postoperative NCP, remain unknown.
WHAT THIS STUDY ADDS
High preoperative mean refractive spherical equivalent and poor preoperative corneal nerve status were significant risk factors for NCP following SMILE, and laser-assisted in-situ keratomileusis, respectively. Tear neuromediators and proteomic changes associated with NCP were also reported.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Patients who are at risk for NCP after refractive surgery can make informed decisions and prophylactic treatment can be administered prior to surgery. The study also provides new insights into the pathophysiological mechanisms of postoperative NCP.
Introduction
Refractive surgery is one of the most common procedures worldwide.1 Despite the excellent visual and refractive outcomes, refractive surgery can negatively impact the ocular surface. While most patients report mild ocular discomfort, a growing number of patients are presenting with persistent ocular symptomatology following refractive surgery,2 such as neuropathic corneal pain (NCP), which can be debilitating.3 As patients undergoing refractive surgery are often young and healthy individuals, and NCP can be detrimental to both vision-related and overall quality of life (QoL),4 it is pertinent to identify the risk factors and patients who are susceptible to these complications so that they can make informed decisions, or prophylactic treatment can be given before the surgery. Patients with NCP experience chronic ocular surface symptoms with minimal or no objective ocular surface staining.4 In-vivo confocal microscopy (IVCM) studies have shown that patients with NCP had a significant reduction in corneal nerve fibre density (CNFD), increased nerve tortuosity, increased frequency of nerve beadings, branching and the presence of neuromas.5
The exact epidemiology of NCP remains to be elucidated, and there have only been a few studies unravelling the incidence of NCP following refractive surgery. In a cross-sectional study of patients seeking consultation for persistent symptomatic dry eye after refractive surgery, 63.5% were diagnosed with chronic neuropathic ocular pain.6 The absence of flap creation in small incision lenticule extraction (SMILE) is thought to reduce flap-related negative impacts such as corneal denervation and postoperative neuroinflammatory responses, as compared with the more well-known laser-assisted in situ keratomileusis (LASIK). However, the phenotypic characterisation of NCP following SMILE remains unknown. Additionally, there is little literature on the molecular profiles of patients with NCP, and none has reported the proteomic data of NCP associated with refractive surgery. While a recent cross-sectional study presented a significantly higher level of nerve growth factor (NGF) in patients with chronic ocular pain following refractive surgery compared to those with dry eye disease and the control group,7 comprehensive molecular data and proteomic profiling are still lacking.
In this comparative clinical study, we investigated the clinical, imaging and tear proteomic characteristics, as well as the risk factors for developing NCP following SMILE and LASIK.
Materials and methods
Study population
This prospective study involved 100 eyes that had undergone bilateral SMILE or LASIK for the treatment of myopia or myopia astigmatism with a spherical equivalent less than −10 D or cylinder <3 D at the Singapore National Eye Centre. Hyperopia was excluded. Patients’ demographic data, pharmacological history, preoperative manifest refractive spherical equivalent (MRSE) and intraoperative data including the cap or flap thickness, size of the optical zone and ablation/treatment zone were recorded. The study was conducted in accordance with the Declaration of Helsinki, and approval for the study was granted by the Institutional Review Board of SingHealth, Singapore (2020/2050/A). All patients provided informed consent to participate in this study.
Surgical procedures
Surgical procedures were performed using a previously described technique by an experienced surgeon (JSM).8 SMILE was performed using a femtosecond laser (Carl Zeiss Meditec, Jena, Germany). A 2.1 mm circumferential incision at 120° was made with the parameters as follows: cap thickness, 100 to 130 µm; mean optical zone, 6.4±0.1 mm; and mean treatment zone, 6.6±0.1 mm. For LASIK, the Visumax laser was used to create a superiorly hinged flap with the following parameters: flap thickness, 100 to 130 µm; mean optical zone, 6.5±0.1 mm; and mean treatment zone, 8.0±0.2 mm. Photoablation was performed using the WaveLight EX500 excimer laser (Alcon Laboratories, Inc, Fort Worth, Texas).
Postoperative treatment included topical preservative-free dexamethasone and moxifloxacin, administered 3-hourly for a week, followed by four times daily for 2 weeks. No topical or oral non-steroidal anti-inflammatory drugs were prescribed.
NCP assessment
Ocular pain assessment survey (OPAS) questionnaires were conducted at 6 and 12 months postoperatively. Each test question was scored on a scale of 0 to 10 or 0 to 100%, with increments of 1 or 10%, respectively. A higher score indicates greater pain intensity. NCP was diagnosed if the patient met all of the following criteria at either 6 or 12 months: (a) the presence of chronic pain or pain-like symptoms with at least three items of >30% in OPAS; (b) abnormal nerve findings on IVCM, typically neuromas defined as ‘abrupt swellings of injured nerve endings and neurite sprouting’. Notably, reduced CNFD or CNFL was not considered as one of the abnormal findings as they would be markedly decreased following surgery; and (c) minimal corneal and ocular surface fluorescent staining (National Eye Institute (NEI) score of <2). All patients with NCP underwent a proparacaine challenge test, which assess the patients’ response to topical 0.5% proparacaine hydrochloride (Alcaine, Alcon, Fort Worth, TX) to establish the origin of pain (peripheral or central).
IVCM scans, image analyses and ocular surface assessments
IVCM scans and ocular surface assessment were performed preoperatively, and at 1, 3, 6 and 12 months postoperatively.
IVCM (Rostock Cornea Module, Heidelberg Engineering GmbH, Germany) was used to evaluate corneal nerve plexus, neuromas and dendritic cells based on standardised published protocols.9 The central cornea was scanned, followed by the nasal, temporal, superior and inferior regions of the cornea at a distance of roughly 3 mm from the corneal apex. For the corneal nerve analysis, the five best-focused images were selected for each area, and each nerve (main trunk or branched nerve) was selected only once. These 25 micrographs selected for each eye were analysed by automated software (ACCMetrics, University of Manchester, UK)10 for the seven nerve parameters listed in table 1. All images for each eye were also manually checked for corneal neuromas. Image J was used for the three neuromas parameters (table 1). Moreover, images with small, bright, dendriform cells,11 termed dendritic cells (DCs), were manually identified. Ten best-quality images containing DCs from each eye were chosen for analysis. The AIConfocal Rapid Image Evaluation System (ARIES; ADCIS, S.A., Saint-Contest, France) was used for the quantification of the five DC parameters (table 1). All IVCM scans were selected by a single investigator (LC) and analysed by an independent investigator (XYL). Both investigators were masked to the surgical procedures and ocular conditions.
Parameters analysed for in-vivo confocal microscopy images
Ocular surface assessments including tear break-up time (TBUT), Schirmer’s I test, corneal sensitivity, ocular surface and corneal fluorescein staining, were performed as previously described.12 For TBUT, three measurements were taken, and the average was used for analysis. Cochet–Bonnet esthesiometer (Luneau Opthalmologie, France) was used to measure corneal sensitivity. The central and four peripheral quadrants were graded on a scale of 0 to 6 cm, with a total scale of 0 to 30 cm. Ocular surface staining was graded using the Oxford grading scale (0–5), and corneal staining was graded using the NEI scale (0–15).
Tear enzyme-linked immunosorbent assay (ELISA) analysis
ELISA was performed as previously described13 preoperatively, and at 1, 3, 6 and 12 months postoperatively. In brief, Schirmer strips were eluted. Sonication and homogenisation were performed, followed by 17 hours of incubation. The homogenisation step was repeated once before centrifugation, and the clear supernatants were collected. Eluted tear samples were analysed for substance P (SP), calcitonin gene-related peptide (CGRP), neuropeptide Y (NPY) and NGF (SP & NGF: R&D Systems, Minneapolis, USA; CGRP & NPY: Phoenix Pharmaceuticals, Rumcorn, UK).
Tear proteomic analysis
Quantitative tear proteomic analysis was performed as previously described14 preoperatively and at 1, 3, 6 and 12 months postoperatively. The Schirmer strips were cut and lysed. The total protein concentration was measured. Eluted tear proteins were reduced, alkylated, tryptic digested and desalted. The total peptide amount was quantified. All peptide samples were analysed using an Orbitrap Exploris 480 Mass Spectrometer via an EASY-Spray Source. Quantitative proteomic analysis was carried out with data-independent acquisition (DIA) experiments. DIA data were processed using library-free direct DIA workflow in Spectronaut 15. The downstream data analysis, data visualisation and Gene Ontology term enrichment were performed using custom scripts in R (64-bit version 4.1.1). The raw abundance data were median-normalised to the total protein concentration of each tear sample and log-transformed for all statistical analyses.
Statistical analysis
Data were expressed as mean±SD with p values of ≤0.05 considered statistically significant. The data from both eyes at the time when NCP was diagnosed were included, and the comparisons between NCP and non-NCP groups, as well as the correlation between two parameters, were analysed using a linear mixed model, to account for correlations of both eyes. Multivariate binary logistic regression analysis was performed for variables that had p values of <0.2 in the univariate binary logistic regression analysis and adjusted for the programmed MRSE, cap or flap thickness, size of the optical zone and size of the ablation/treatment zone, to determine the significant risk factors for the development of NCP. The sample size was calculated based on the formula: n=100+50 i, where ‘n’ refers to the number of patients times total visits and ‘i’ refers to the number of independent variables in the multivariate model.15 All the statistical analyses were performed using STATA software (Version 17, STATACorp, College Station, TX).
For the proteomic data, principal component analysis (PCA) and sparse partial least-squares discriminant analysis (sPLS-DA) were performed to visualise the differences in (1) two-group comparisons, non-NCP vs NCP groups, and (2) three-group comparisons, non-NCP after either surgery vs NCP after LASIK (NCP/LASIK) vs NCP after SMILE (NCP/SMILE).
Results
Patients’ demographics, refractive parameters and preoperative data
The study involved 100 eyes, equally divided between SMILE and LASIK procedures, with a mean patient age of 30.6±6.0 years. The majority were females (69.0%). Of these, six eyes (13.3%, 95% CI: 5.1—26.8%) developed NCP after SMILE, and four eyes (10.5%, 95% CI 2.9—29.8%) developed NCP after LASIK, with no significant difference in incidence between the groups (p=0.70). Specifically, NCP was diagnosed at 6 months for two SMILE eyes and two LASIK eyes; and at 12 months for four more SMILE eyes and two more LASIK eyes. All patients in the NCP group had bilateral peripheral NCP. Patients with NCP after SMILE had a significantly higher preoperative MRSE (NCP/SMILE: −8.7±1.8 diopters (D) vs non-NCP/SMILE: −5.8±2.7 D, p=0.02) and spherical power (NCP/SMILE: −7.7±1.8 D vs non-NCP/SMILE: −5.2±2.5 D, p=0.02; table 2). The preoperative IVCM findings, ocular surface parameters, and tear neuromediator concentrations are presented in online supplemental table 1). None of the patients were on centrally acting neuromodulators, such as antiepileptics or antidepressants, and one non-NCP/LASIK patient was on antihistamines.
Supplemental material
Demographics and clinical parameters of study participants
IVCM parameters
Postoperative eyes presented with nerve beadings and three types of neuromas: stump, fusciform and lateral neuromas16 (figure 1).

Representative in-vivo confocal microscopy images of the corneal nerves and different types of neuromas in patients with neuropathic corneal pain (a) nerve beading (arrow), characterised by small, bead-like enlargements along the length of corneal nerves; (b) stump neuromas (arrows), which appeared as abrupt and swollen termination of the stromal nerves; (c) fusiform neuroma (left arrow), a hyperreflective fusiform enlargement along the nerve trunk without axonal sprouting and stump neuroma (right arrow, described in (b)); (d) lateral neuroma (right arrow), characterised by the localised hyperreflective enlargement of nerve from which single, or multiple tortuous nerves sprout, and stump neuroma (left arrow; described in (b)); (e) lateral neuroma (arrow, described in (d)).
Among the patients who underwent LASIK, those with NCP had a significantly higher CNFW (p=0.04) and a significantly lower CNFL and CFracDim (p=0.02 and p=0.003, respectively). CNFD was observed to be borderline significantly lower in the NCP group following LASIK (p=0.06). The total area of neuroma was significantly larger in post-LASIK patients with NCP as compared with those without NCP (p=0.04). These differences were not seen in the post-SMILE eyes. DCs parameters showed no significant differences in either group (table 3). When comparing between the patients who underwent LASIK and SMILE, the post-LASIK eyes had significantly worse CNFD (p<0.00001), CNBD (p=0.0001), CNFL (p<0.00001), CTBD (p=0001), CNFA (p=0.0003), CNFW (p=0.01) and CFracDim (p<0.00001) compared with the post-SMILE eyes (online supplemental table 2). There was no significant difference in DCs or neuroma parameters (online supplemental table 2).
Supplemental material
In-vivo confocal microscopy, ocular surface, tear neuromediator parameters at the time neuropathic corneal pain was diagnosed
Ocular surface assessments
After LASIK, all ocular surface parameters were comparable between the patients with and without NCP. In SMILE, the NCP group had a significantly higher Oxford and NEI staining scores, but the overall staining was minimal (table 3). Post-LASIK eyes also exhibited significantly higher Oxford and NEI staining scores compared with post-SMILE eyes. There was no significant difference in the other ocular surface parameters between the two surgical techniques (online supplemental table 2).
Pain assessments
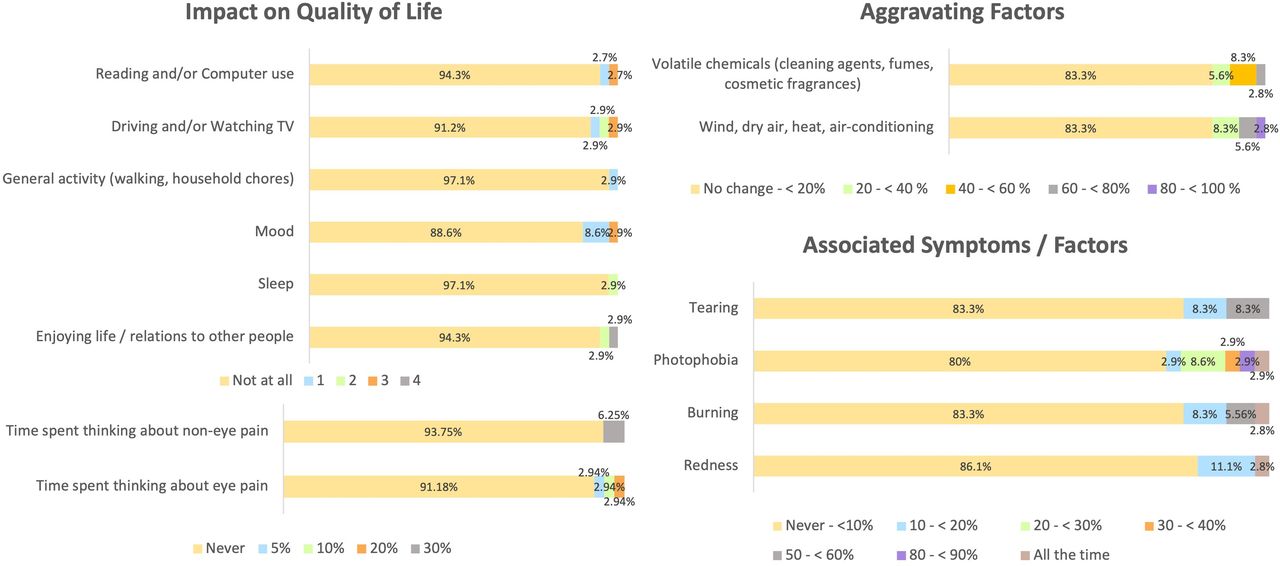
NCP patients reported significantly higher ocular symptoms, including redness (p=0.02), burning (p=0.001), sensitivity to light (p=0.005) and tearing (p=0.01). Photophobia was the most common symptom, reported by 80% of NCP patients. Notably, QoL was also significantly impacted by NCP as compared with those without NCP, affecting (a) driving and/or watching TV (p<0.001), (b) general activity (p=0.01), (c) mood (p<0.001), (d) sleep (p=0.02) and (e) enjoying life/relations to other people (p<0.001). Participants’ responses for the OPAS questionnaire are shown in figure 2.

Ocular pain assessment survey responses of study participants including impact on the quality of life, aggravating factors of pain and associated symptoms/factors.
Tear neuromediator concentrations
At 1 year postoperatively, regardless of the surgical type, tear NGF and CGRP levels were significantly higher in patients with NCP than those without NCP (all p<0.05; table 3). NCP/LASIK had significantly higher SP (p<0.001) and NPY (p=0.004) levels than non-NCP/LASIK (table 3). There was no significant difference in the tear neuromediator concentrations between the two surgical techniques (online supplemental table 2).
Risk factors associated with the development of NCP
In the univariate regression model, lower preoperative CNFA (p=0.04), higher preoperative tear CGRP level (p=0.04) and higher preoperative MRSE (p=0.01) were associated with the development of NCP after SMILE. After adjusting for all other covariates in the multivariate regression, preoperative MRSE remained a significant risk factor (95% CI: 0.48 to 1.96, p=0.04) (table 4). Eyes with a preoperative MRSE greater than −8.0 D had a 9.57 times higher likelihood of developing NCP [OR=9.57, 95% CI: 2.21 to 41.4, p=0.002).
Univariate and multivariate regression analyses for factors associated with the development of neuropathic corneal pain after small incision lenticule extraction
In the post-LASIK eyes, lower preoperative CNFD (p=0.02) and CNFL (p=0.001) were significantly associated with the development of NCP, both in the univariate analysis, and adjusted model in multiple testing (95% CI: 0.13 to 1.11, p=0.049 and 95% CI: 0.09 to 1.25, p=0.046, respectively, table 5).
Univariate and multivariate regression analyses for factors associated with the development of neuropathic corneal pain after laser-assisted in-situ keratomileuses
Tear proteomic analysis
The volcano plot represents the proteins that are significantly up- and down-regulated in the NCP group (figure 3a). On PCA and sPLS-DA analyses, there was good separation with minimum overlap between the NCP and the non-NCP group, suggesting the existence of significant differences. The separation of the NCP and non-NCP group was mainly driven by several tear proteins including Frizzled class receptor 7 (FZD7), nucleoside-diphosphate kinase 3 (NME3), Alkaline phosphates tissue-nonspecific (ALPL), Tight Junction Protein 2 (TJP2), Interleukin 1 Receptor Antagonist (IL1RN), Thioredoxin (TXN), apolipoprotein B (APOBEC3A), and Ttarget of Myb1 Membrane Trafficking Protein (TOM1) (figure 3b). Further discrimination between the non-NCP/SMILE, non-NCP/LASIK, NCP/SMILE and NCP/LASIK groups was demonstrated by sPLS-DA (figure 3c). FZD7 and NME3 remained as significant proteins expressed in the NCP/SMILE group. In the NCP group, FZD7 and NME3 were significantly upregulated, whereas TOM1, APOBEC3A, ALPL, TJP2, IL1RN and TXN were significantly downregulated (figure 3d).

{kind=link}
{kind=link}
{kind=link}
Tear proteomic changes associated with neuropathic corneal pain (NCP). (a) Volcano plots presenting the fold changes of tear proteins comparing NCP with non-NCP group. Log2 Fold Change (FC) of >0.5 represents proteins that are upregulated, and Log2 FC <−0.5 represents proteins that are down regulated, with p<0.05, −log10 p value >1.3 as significant. (b) Principal component analysis plot showing the separation of NCP and non-NCP group. Separation between both groups were mainly driven by Frizzled class receptor 7 (FZD7) and nucleoside-diphosphate kinase 3 (NME3); (c) sparse partial least-square discriminant analysis plot showing the discrimination between the four subgroups. (d) Box and whisker plots showing the significant upregulation and downregulation of tear proteins in patients with NCP vs those without NCP. FZD7 and NME3 are significantly upregulated, and alkaline phosphates tissue-nonspecific (ALPL), Tight Junction Protein 2 (TJP2), Interleukin 1 Receptor Antagonist (IL1RN), Thioredoxin (TXN), Apolipoprotein B (APOBEC3A) and Target of Myb1 Membrane Trafficking Protein (TOM1) are significantly downregulated in patients with NCP compared with those without NCP.
Discussion
This study identified key risk factors for NCP after refractive surgery: greater preoperative MRSE in SMILE, and poorer preoperative nerve metrics in LASIK. Regardless of the surgical type, tear NGF, CGRP, FZD7 and NME3 levels were significantly elevated in patients with NCP.
The incidence of NCP was 13.3% in SMILE and 10.5% in LASIK, comparable to a recent study reporting that 11% of participants experienced persistent ocular pain following refractive surgery.17 The same study presented preoperative ocular pain, depressive symptoms and antiallergy medication usage as significant risk factors for postoperative persistent ocular pain (not limited to neuropathic origin).17 Another study found that neuropsychiatric conditions and central sensitisation syndromes put patients at a higher risk of developing post-refractive surgery NCP.18 To the best of our knowledge, no study has investigated the risk factors that render patients more susceptible to NCP following SMILE. Our findings show that patients with a preoperative MRSE greater than −8 D were 9.57 times more likely to develop NCP. Following corneal nerve disruption during surgery, peripheral sensitisation arises from increased responsiveness of nociceptors. The transduction mechanism at the corneal nociceptors converts external stimuli into electrical impulses that travel through the trigeminal nerve. These impulses then follow the corneal pain pathway, which includes the trigeminal brainstem complex, cervical cord and thalamus, before being processed in the cerebral cortex. Amplified input from peripheral nerves triggers hyperexcitability in central nociceptors.19 Additionally, inflammatory mediators and neuromediators cause an influx of leucocytes in the cornea, further perpetuating existing inflammation.20 ,21 These maladaptive processes contribute to persistent neuropathic pain. Our group has previously reported that corneal denervation increased when the corrected refractive power increased in SMILE, as an increase in the refractive power corrected led to an increase in the extracted lenticule’s total neurite length.22 Additionally, high myopia correction has more stromal tissue devoid of keratocytes, which decreases keratocytes’ ability to provide biological and nutritional cues for nerve regeneration.23 These findings thus support the conclusion that corneal denervation is greater in those with a higher preoperative MRSE, thereby leading to a greater extent of neuroinflammation and resultant NCP.22 For LASIK, we found patient’s preoperative nerve status to be significantly associated with postoperative NCP. Nerve fibres were found to decrease by >90% immediately after LASIK,24 and reinnervation following LASIK was slower than SMILE and PRK.21 Therefore, if preoperative nerve density is lower and nerve fibres were shorter to begin with, the remaining nerve bundles are expected to be significantly lower postoperatively than those with a better preoperative nerve status. Decreased nerve fibres also reduce the trophic factors that maintain corneal haemostasis, rendering patients more susceptible to postoperative NCP.25 Interestingly, our study found no significant association between preoperative corneal nerve metrics and postoperative NCP in SMILE. We postulate that a poorer preoperative nerve status may be more forgiving following SMILE because nerve truncation is comparatively minimal, and subsequent reinnervation occurs more quickly than with LASIK.21 In both types of surgery, preoperative ocular surface parameters were not risk factors. This might be because patients’ ocular surface should be and have been optimised preoperatively.
On IVCM evaluation, patients who developed NCP had significantly lower CNFL, higher CNFW, lower CFracDim and greater neuroma areas in the LASIK group. Patients with NCP were shown to have significantly reduced CNFL and CNFD as well as greater nerve tortuosity compared with controls.26 Several studies have also reported that patients with NCP had a substantial number of neuromas.16 Neuromas are caused by the disruption and subsequent regeneration of nerve fibres, causing ectopic firing, explaining the hyperalgesia.27 The aforementioned significant nerve findings were not found between our NCP/SMILE and non-NCP/SMILE cohort, but a trend was still observed. This might be a result of more nerve being preserved in SMILE21 In this study, lower corneal nerve metrics in the post-LASIK eyes compared with post-SMILE eyes were also observed. There was no significant difference in all the neuroma parameters, as well as the incidence of NCP, between LASIK and SMILE. These might suggest that corneal neuromas are more relevant to NCP. In terms of the DCs parameters, there was no significant difference between the NCP and non-NCP eyes, which is consistent with previous findings that the DCs density between NCP and healthy controls was not significantly different.28 This finding could also be accounted for by the suppression of DCs’ activities following postoperative topical steroid use. Although IVCM is not routinely performed before refractive surgery, our study suggests it can be considered for a select group of high-risk patients, such as those undergoing high myopic treatment.
The most frequently reported symptom in our NCP cohort was light sensitivity. Several photophobia circuits related to pain and somatosensation have been proposed, but the underlying mechanism is still poorly understood. Noseda et al identified that convergent input from trigeminal and retinal afferents on the same thalamic neurons makes them uniquely positioned to interpret light as nociceptive signal. Pathologic central sensitisation within the trigemino-cortical nociceptive pathway has also been reported to contribute to photophobia.29
In the present study, NCP/SMILE and NCP/LASIK eyes demonstrated significantly higher tear NGF and CGRP levels. NGF is considered to be an endogenous mediator in persistent pain states, and evidence for this critical function in the development of pain and hyperalgesia is growing. It has been demonstrated that subjects experienced hyperalgesia after subcutaneous injection of NGF.30 CGRP plays a part in neurogenic inflammation and transmission of pain.31 NCP/LASIK eyes also had significantly higher tear concentrations of SP and NPY than non-NCP/LASIK eyes. SP and NPY are known for modulating neuroinflammation and neurotransmission.32 Due to a lesser extent of neuroinflammatory and inflammatory reactions in SMILE,14 SP and NPY were not significantly increased in NCP/SMILE when compared with the non-NCP/SMILE group.
Importantly, there is still much that is unexplored in the molecular mechanisms underlying the pathogenesis of NCP after refractive surgery. In this study, we found FZD7 and NME3 to be significantly elevated in NCP. Frizzled genes are essential for the regulation of neuronal differentiation, axonal growth and neuronal plasticity.33 In particular, FZD proteins are known as the receptor for the wingless-related integration site (Wnt) signalling pathway, which is critically involved in neuropathic pain.34 The injection of Wnt3a inhibitor significantly increased the mechanical pain threshold in rats, and activation of the Wnt/β-catenin pathway induces neuropathic pain by enhancing neuronal excitability.35 NME3 plays a major role in the stimulation of mitochondrial fusion.36 Since the energy demand for synaptic transmission relies on mitochondrial motility across long distances in neurons, our data suggest a possible link between NME3 and NCP development. We also found TOM1 to be significantly downregulated in the NCP group. Reduced TOM1 has been shown to negatively affect neuronal internalisation.37 Our results demonstrate that the downregulation of TOM1 could have thus accentuated neuroinflammation in NCP.
There are several limitations in this study. First, the study participants who underwent SMILE had higher preoperative MRSE, as compared with those who underwent LASIK. In our centre, SMILE is preferred for the treatment of high myopia as studies have shown that SMILE delivers greater refractive predictability for high myopic correction.38 Therefore, the significant relationship between preoperative MRSE and NCP might be difficult to be discern in the LASIK group. Second, the OPAS questionnaires were conducted only at 6 and 12 months postoperatively. This timeframe was chosen because the onset of post-refractive surgery ocular pain was reported to occur 9.6 months postoperatively.18
In conclusion, we discussed the factors that put patients at risk for postoperative NCP following SMILE, in addition to LASIK. Identification of risk factors would allow for the early recognition of patients at risk of this debilitating and persistent complication. Due to the paucity of data on the clinical, imaging and proteomic profiles of patients with postoperative NCP, our findings provide a comprehensive knowledge of the components that enhance patients’ susceptibility to developing post-surgical NCP. The proteins and neuromediators identified would also serve as potential biomarkers or therapeutic targets for NCP following refractive surgeries.
Data availability statement
Data are available upon reasonable request. Data will be made available upon request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the Institutional Review Board of SingHealth, Singapore (2020/2050/A). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The bioinformatics analysis was supported by InnoHK initiative and the Hong Kong Special Administrative Region Government and PolyU SHS grant (P0043882).
References
Footnotes
Contributors CHYT: conceptualisation, writing – original draft, formal analysis, data curation, visualisation. CL: investigation. IXYL: data curation, visualisation. MTYL: data curation, visualisation. FYL: data curation. CJLT: data curation, KSK: investigation. DQL: investigation, visualisation. TCL: investigation. ZL: formal analysis, data curation, visualisation. LT: writing – review and editing. JM: investigation, writing – review and editing. Y-CL: conceptualisation, methodology, writing – review and editing, formal analysis, data curation, supervision, funding acquisition. YC-L is the guarantor of this study.
Funding This work was supported by the grant from the Singapore National Medical Research Council [MOH-CSAINV21jun-0001]
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.